
MEDICAL ARTICLES

The Mechanism of Shoulder Pain in Aquatics
Farhad Moradi Shahpar MD., FINA SMC Member
Mojtaba Ebrahimi Varkiani MSc, University of Tehran
Jim Miller MD, FINA SMC Member
Saul Marks MD, FINA SMC Honorary Secretary
Shoulder pain is the most common musculoskeletal complaint that affects competitive swimmers. In one study, over 34% of swimmers sustained shoulder injuries that led to more than 30 days off training. One of the first reports of this problem was in the 1972 Olympic Games in Munich when a high incidence of shoulder pain was noticed among 35 Canadian competitive swimmers. There were 43 orthopedic consultations, with 16 specific-related to shoulder (37%) as the most frequently experienced problem. The fact that swimmers experience shoulder pain is not surprising. During training and competition swimmers can complete over 1 million shoulder rotations per year. T Murphy TC (1994) Murphy et al calculated that swimming is equated to running for energy expenditure in a ratio 1:4 in that running 4 miles is equivalent to swimming 1 mile. Therefore, this type of training predisposes swimmers to overuse injuries of the shoulder.
Although athletes in overhead sports such as baseball, tennis, volleyball, and water polo are susceptible to shoulder pain, the high incidence of shoulder pathology in swimmers has resulted in use of the term “Swimmer’s Shoulder.”
Shoulder pain in swimmers is often caused by impingement. Impingement is now a widely used term to describe a situation that occurs when the space between the humeral head and the acromion, known as the sub-acromial space, becomes narrowed. In these situations the bones can then “impinge,” or squeeze, the structures that occupy this space.

Diagram 1 – Shoulder Anatomy – sub-acromial space
Sub-acromial space
The sub-acromial space is situated below the acromion of the scapula and above the upper aspect of the ball of the humerus. (see Diagram 1) Specific tissues that occupy a portion of this space include the supraspinatus tendon, the sub-acromial bursa, the long head of the biceps tendon and the shoulder capsule. Maintaining a sub-acromial space that has room for freedom of movement is critical to shoulder health due to the many contained structures that lay within. Sub-acromial impingement (SAI) typically precedes rotator cuff disease, and exists when this space is decreased and tissues are compressed. Of particular concern is the supraspinatus tendon, which is generally the site of initial rotator cuff injuries. (see diagrams 2 and 3)

Diagram 2 – Muscles of the Rotator Cuff
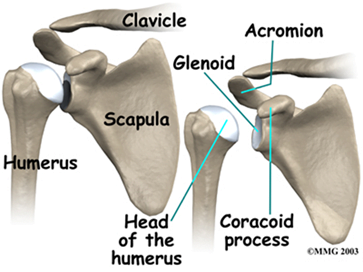
Diagram 3 – Bones of the Shoulder Joint
Under training conditions, the tendon accumulates water and inflammatory proteins. The tendon fibers fray and become disorganised resulting in the tendon thickening. These structural changes also result in decreased elasticity in the tendon, requiring less pull or stress on the tendon for it to rupture.
The shape of the acromion itself, which varies from person to person, impacts impingement. Acromial shape is described in three ways: Type I: flat, Type II: curved, and Type III: hooked, and has been associated with the likelihood of impingement. Each of the three types are shaped exactly as they sound. With Type I the acromion is flat, with Type II the acromion is curved, while Type III is “bent” or “hooked”. In fact, acromion shape has been reported as a high internal predictor of future impingement and rotator cuff tears, especially for Types II and III.
There are two major theories about the causes of impingement.
1 – Superior humeral movement: This theory supposes that upward motion of the humeral head decreases the sub-acromial space. If the rotator cuff cannot maintain correct positioning of the humeral head, the head moves up in the socket, causing impingement.
2 – Scapular movement disorder: This theory supposes that weak or dysfunctional muscles (i.e. after fatigue) results in improper scapular movement, resulting in a reduction of the sub-acromial space.
Both of these theories may be related to shoulder instability. Imbalances of the rotator cuff musculature, excess capsular looseness, or loss of posterior capsular flexibility have all been implicated as causes of both shoulder instability and impingement syndrome. This may result in repeated micro trauma in the soft tissues of the shoulder, which can ultimately lead to failure of the supporting structures.
Mechanisms of injury in swimming
The human body is created to move on feet, therefore when we try to move by our hands in the water, we have to face against some resistance or “drag”, which can be active or passive. Passive resistance is experienced by a swimmer’s body during passive towing, exposure to water flow in a flume, or performing gliding without movements. Active resistance is experienced during swimming and combines passive resistance of the core body with additional wave-making and eddies caused by swimming movements. There are three forms of drag that occur as swimmers moving through the water.
1) Form Drag (Passive):
The most streamlined posture is the gliding posture in which the body and legs are outstretched, the toes are pointed, the arms are stretched over the head and hands topping one another and the ears are pressed by the shoulders. Even minor deviations of the head, arms and legs from a streamlined position during the glide after starts and turns may result in a considerable increase of resistance.
2) Frictional Drag (Passive):
This drag occurs by the very fact that the swimmer is in water. During swimming the water coating the body surface ‘sticks’ to it and travels with the same speed as the swimmer. The more surface area of the body that is submerged in the water, the more the Frictional Drag.
3) Wave Drag (Active):
This drag occurs from the resistance produced by the swimmer when he or she executes the swimming stroke. The refined technique of elite swimmers gives them much less active drag (AD) than average swimmers over a range of swimming velocities. Thus the reduction of AD should become a target for stroke development in swimming.
These drag forces become amplified with improper stroke technique. In particular, technique in three phases of the swimming stroke can affect drag and as result, increase the likelihood of shoulder impingement. The explanations of these phases below reference the front crawl stroke, since that stroke typically occupies a large percentage of swim training.
The “catch” phase (arm entry to the water)
During the initial extension of the arm and “catch” phase of the front crawl swimming stroke the shoulder and the arm are forcibly elevated. This action causes the head of the humerus to move under the arch of the sub-acromial space, can lead to potential impingement of the structures that lie in this space discussed above.
The “catch” and pull phase
During the pull phase the shoulder moves away from the body but rotates inward. This results in the arm following an inverted question mark pattern under the water. One of the most common technical faults during this phase is the “dropped elbow”. Dropping the elbow during the pull phase causes increased unwanted outer shoulder rotation. In addition, too much movement of the hand and arm past the midline during the pull phase can cause inward rotation of the shoulder which may present yet another mechanism for causing impingement of the structures that lie in the sub-acromial space.
The recovery phase
Following the pull phase the arm leaves the water usually elbow first (elbow lift) and is required to undergo a recovery phase. The recovery phase is one of the more important phases in terms of risk for possible shoulder impingement and injury. The shoulder is required to rotate up and out to clear the arm over the water, then quickly to prepare for the arms extension and entry to the “catch” phase position.
The timing of this rotation and the magnitude of this action during the recovery is a critical component of risk associated with shoulder impingement. It has been shown that swimmers who execute the recovery phase with a large amount of initial inward rotation rather than outward rotation of the shoulder are susceptible to potential increased shoulder impingement as discussed above. These repetitive forces may result in further anatomical changes in the shape of the acromion, if they are not already there.
Summary
Impingement is a widely used term describing the events contributing to the common problem referred to as a “Swimmer’s Shoulder.” It is important to consider the structures within the shoulder that are susceptible to being pinched as well as the circumstances under which an athlete is subjected to increased risk. The joint capsule, the tendons of the rotator cuff and the sub-acromial bursa are placed at risk of “being compressed.” This compression can make tendons thicken and become less elastic, thus increasing the possibility of tendon rupture. Different aspects within stroke technique, most notably the recovery and the catch, can place the joint capsule, the tendons of the rotator cuff and the sub-acromial bursa at risk of injury and must be considered in stroke development to lessen the risk.
Four Key Points
- Swimmers Shoulder is the most common musculoskeletal complaint in the sport of swimming.
- Shoulder impingement is caused by a lack of room in the sub-acromial space, effecting the supraspinatus tendon, the sub-acromial bursa, the long head of the biceps tendon and the shoulder capsule.
- Correct swimming technique can reduce the risk of developing Swimmer’s Shoulder
- One benefit of improved technique is less Active Drag which can reduce stress on the shoulder.
Questions
- What are four structures that occupy the sub-acromial space and are susceptible to being pinched?
- What can occur when the sub-acromial space is compressed?
Answers
- The supraspinatus tendon, the sub-acromial bursa, the long head of the biceps tendon and the shoulder capsule.
- Sub-acromial impingement (SAI) typically precedes rotator cuff disease. . Of particular concern is the supraspinatus tendon.